Endocrine medications
Oral anti hyperglycaemic medications
In general, these should be taken as normal on the day before the procedure, but not taken on the day of surgery. Local protocols often apply in a hospital. The Beacon Hospital uses a document no. PPS-ORG-68 on Qpulse, “Adult Patients with Diabetes Undergoing Surgery and Elective Procedures”.
Meglitinides
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Examples: Nateglinide, Repaglinide
Metformin
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Sulfonylureas
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Examples: Glibenclamide, Gliclazide, Glimepiride, Glipizide, Tolbutamide
Thiazolidenones
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Example: Pioglitazone
Dipeptidylpeptidase-4 (DPP-IV) Inhibitors (Gliptins)
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Examples: Alogliptin, Linagliptin, Saxagliptin, Sitagliptin, Vildagliptin
Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists
Take the day before the scheduled procedure, but do not take on the day of the procedure.
Examples: Dulaglutide, Exenatide, Liraglutide, Lixisenatide, Semaglutide
Sodium-glucose co-transporter-2 (SGLT-2) InhibitorsGLT-2 inhibitors (gliflozins)
This medication should be held for 72 hours before surgery if the procedure is classified as major or major+/complex.
Examples: Canagliflozin, Dapagliflozin, Empagliflozin, Ertugliflozin
Acarbose
Take the day before the scheduled procedure, but do not take on the day of the procedure.
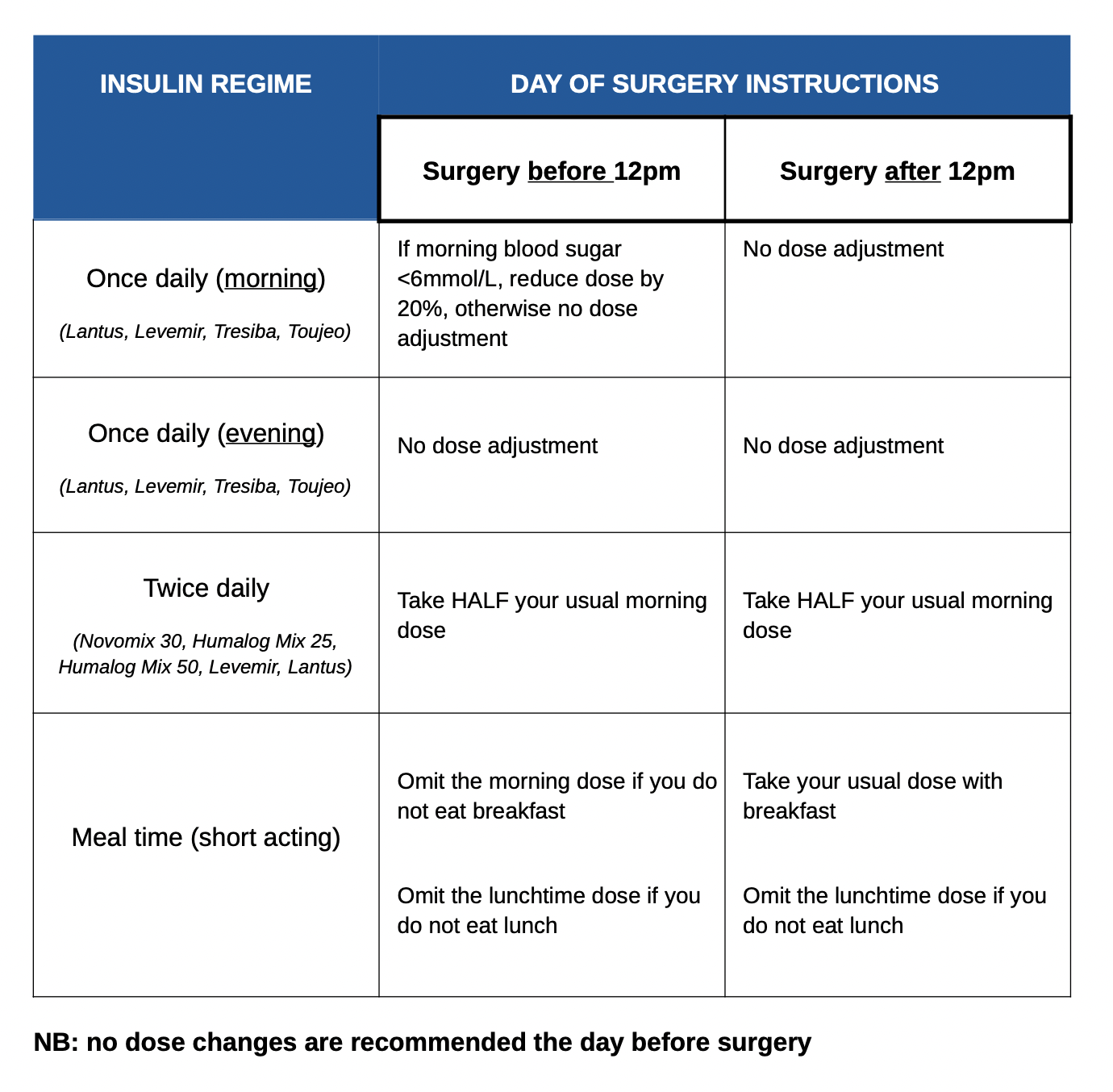
Insulins
Adjustments to a patient’s insulin regime is dependent of the nature of the regime itself. Locl protocols often apply. For example, in The Beacon Hospital, see doc no. PPS-ORG-68 on their Q-Pulse system, “Adult Patients with Diabetes Undergoing Surgery and Elective Procedures”.
Corticoteroids (systemic)
Patients should receive their usual pre-operative dose of steroids on the day of surgery1.
Abrupt withdrawal should be avoided in patients who have received systemic corticosteroids at the equivalent dose of prednisolone ≥ 10mg for longer than 3 weeks2.
Inform the anaesthesiologist for the patient’s list that chronic high-dose steroid use has been identified, ‘stress-dose’ steroids are likely indicated intra-operatively.
Examples: Betamethasone, Budesonide, Deflazacort, Dexamethasone, Fludrocortisone, Hydrocortisone, Methylprednisolone, Prednisolone, Triamcinolone